Anatomy of First Aid: A Case Study Approach
Ronald Bergman, Ph.D.
Peer Review Status: Internally Peer Reviewed

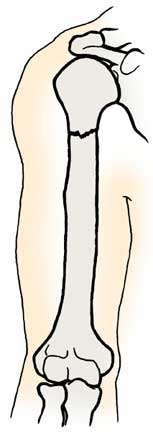
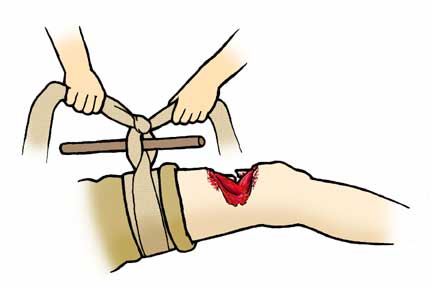
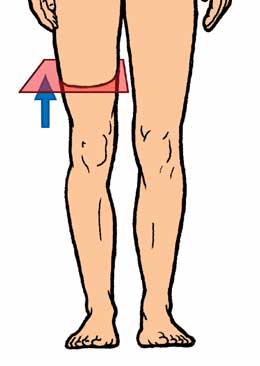
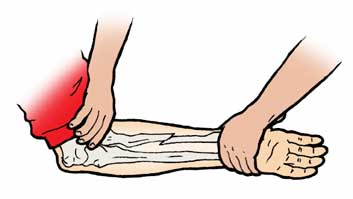
On an aircraft carrier in the Persian Gulf, flight deck personnel were readying fighter aircraft for a strike at enemy ground forces. One of the Sailors had a problem with ordinance and one rocket accidentally discharged. The rocket flew into and past another Sailor causing severe injury to his thigh and fracturing his femur. Ruptured femoral vessels poured forth blood and the injured Sailor fell to the deck unconscious. An alert Sailor called for someone to summon the corpsman and then he dropped to the deck to close off the blood loss by use of a tourniquet. Very shortly afterwards the corpsmen arrived. The corpsman checked the tourniquet (see accompanying illustrations), and wrote on the forehead of the victim the time of application of the tourniquet. The Sailor was covered with a blanket to reduce the possibility of severe shock and the wound was covered with sterile, moist gauze. The injured Sailor's vital signs were taken (pulse, blood pressure and respiratory rate) as he was taken rapidly to the sickbay. In the meantime, the naval surgeon was summoned to sickbay, which was readied for treatment of the injured Sailor. If this accident had happened on shore, the corpsman would have followed the same procedures but would have had to immobilize the leg with a splint. The splint, in combat, might include a branch of a tree or any other inflexible object (preferably clean) a pillow, magazine or newspaper as the supporting structure. The two legs can be merely bound together. The rationale is to avoid causing further damage by the sharp edges of the fractured bones moving about while the patient is being evacuated.
The following are useful guidelines when one considers the possibility of broken bones. A corpsman may use the following signs as indicators of broken bones:
1. Pain or soreness over a joint or bone.
2. The victim tells the corpsman that he heard or felt a break.
3. The victim can't move an injured part or that a move is painful.
4. The victim tells the corpsman that there is numbness or tingling in the injured limb. This is also an indicator of possible nerve injury.
5. An arterial pulse cannot be found in the injured part or limb. This is an indicator of blood vessel injury.
6. The corpsman sees swelling or bruising in the injury site. This an indicator of extravasated blood.
7. The injured part is in an unusual or abnormal position and any possible movement is abnormal.
How to provide first aid to victims with bone or joint injuries? Without x-rays or MR imaging it is not always possible to know if a bone is broken, a joint is dislocated or damaged, or if ligaments are stretched or torn. The rule-of-thumb therefore, is not to guess, but to immobilize the injured part. However, this is not the first step in the first aid of these victims.
1. Treat for any life-threatening condition first: check breathing, pulse and for any bleeding. Finally stabilize the fractured bone or injured joint.
2. It is essential to keep movement of the individual and the injured part to a minimum. The rational for minimal movement is to reduce the possibility of additional damage to bone, muscle, blood vessels and nerves and the production of additional pain.
3. Immobilize the injured part with bandages, slings and splints.


4. If there is torn skin avoid contamination of exposed underlying structures using sterile compresses. Infections of bone are very serious and difficult to treat. If there is a compound or open fracture (bone sticking through the surface of the skin) never try to push the bone inside the torn muscle.
5. Swelling of joints can be avoided by cooling the injured part using ice wrapped in a cloth or towel.
6. Treat for shock and secure the aid of a medical corpsman and physician as soon as possible.

|
Colle's fracture |
|
|
Comminuted fracture |
|
|
Green-stick |
|
|
Impacted |
|
|
Incomplete |
|
|
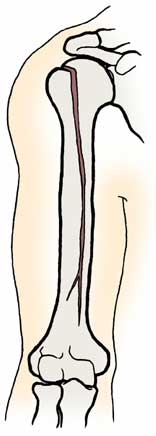
Linear |
|
|
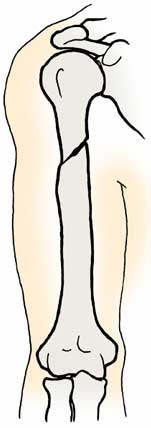
Oblique |
|
|
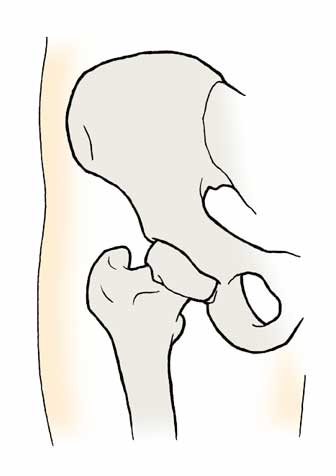
Pott's fracture |
|
|
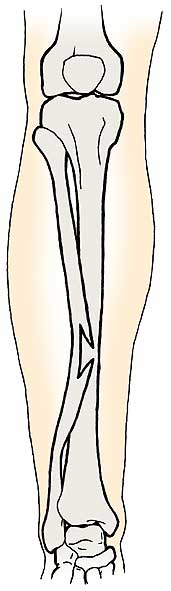
Spiral fracture |
|
|
Transverse fracture |
|



Please send us comments by filling out our Comment Form.
Anatomy Atlases is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License. 
"Anatomy Atlases", the Anatomy Atlases logo, and "A digital library of anatomy information" are all Trademarks of Michael P. D'Alessandro, M.D.
Anatomy Atlases is funded in whole by Michael P. D'Alessandro, M.D. Advertising is not accepted.
Your personal information remains confidential and is not sold, leased, or given to any third party be they reliable or not.
The information contained in Anatomy Atlases is not a substitute for the medical care and advice of your physician. There may be variations in treatment that your physician may recommend based on individual facts and circumstances.
URL: http://www.anatomyatlases.org/